Recommendations for a solution
The above-mentioned legal- and professional problems attest to the fact that regarding the professional health care educational system, the suitable professional development of the professional educational programs according to the specialties regarding the sector – according to the requirements determined by the National Ministry of Economy – was not possible. Therefore it is justified to develop the professional content of the sectoral professional qualifications on a sectoral level, on the examples of the agricultural- and defense professional educational programs. Aside from that, certain educational programs are needed to be taken out from the vocational education (e.g. practicing nurse, nurse), and organize them as a part of higher education (e.g.: as associate degree education, as dual education). By incorporating the appropriate skills and acceptable learning outcomes from the associate degree education to Bachelor nurse education, and by the substantive shortening of the education period, acquiring a Bachelor nurse’s degree in 2,5 years instead of 4 years becomes possible, if the determined subjects of the associate degree education are completed by the student with an at least average mark.
Our aim is the establishment of an EU-conform vocational qualified nurse education of suitable standard applicable for mass- education by correcting the legal errors stemming from the non-compliance to the EU directive regarding the vocational qualified nurse and the professional errors stemming from the bad structure of the professional high school system, with the coordination of the universities, making it able to be incorporated in higher education. During the incorporation of vocational health care educational programs (e.g. nurse) into the Bachelor’s education, the associate degree education programs are suggested to be organized by county in one (in case of need, several) vocational educational institution, which was maintained by the higher educational institution faculty operating in the given region. This practice was properly functioning from the 1920’s to the 40’s, when the Hungarian Royal National Nurse- and Health Visitor Educational Institutions were functioning within the Universities.
Some authors of the present study and the Hungarian Scientific Society of Nursing and have repeatedly initiated the transformation of public education in the past 8 years. We are pleased to find it in sync with the government's endeavor to bring institutions of state-run to come under the maintenance of health care related higher educational institutions. We need to support this process in order to increase the number of applicants and entrants to health care skill shortages to compensate the lack of professionals. The national data for the past 10 years also supports the viability of the “Vocational Education Model of Pécs”, as against a steady and significant decline the number of students in school-based education in health care dropped from 2009 to 2018 from 8,200 to 4,000 in the number of students in institutions of state-run vocational education institutions, the number of students applying to the University of Pécs, Social and Health Care Vocational High School (PTE SZESZI) during this period has tripled in Baranya and Vas counties.
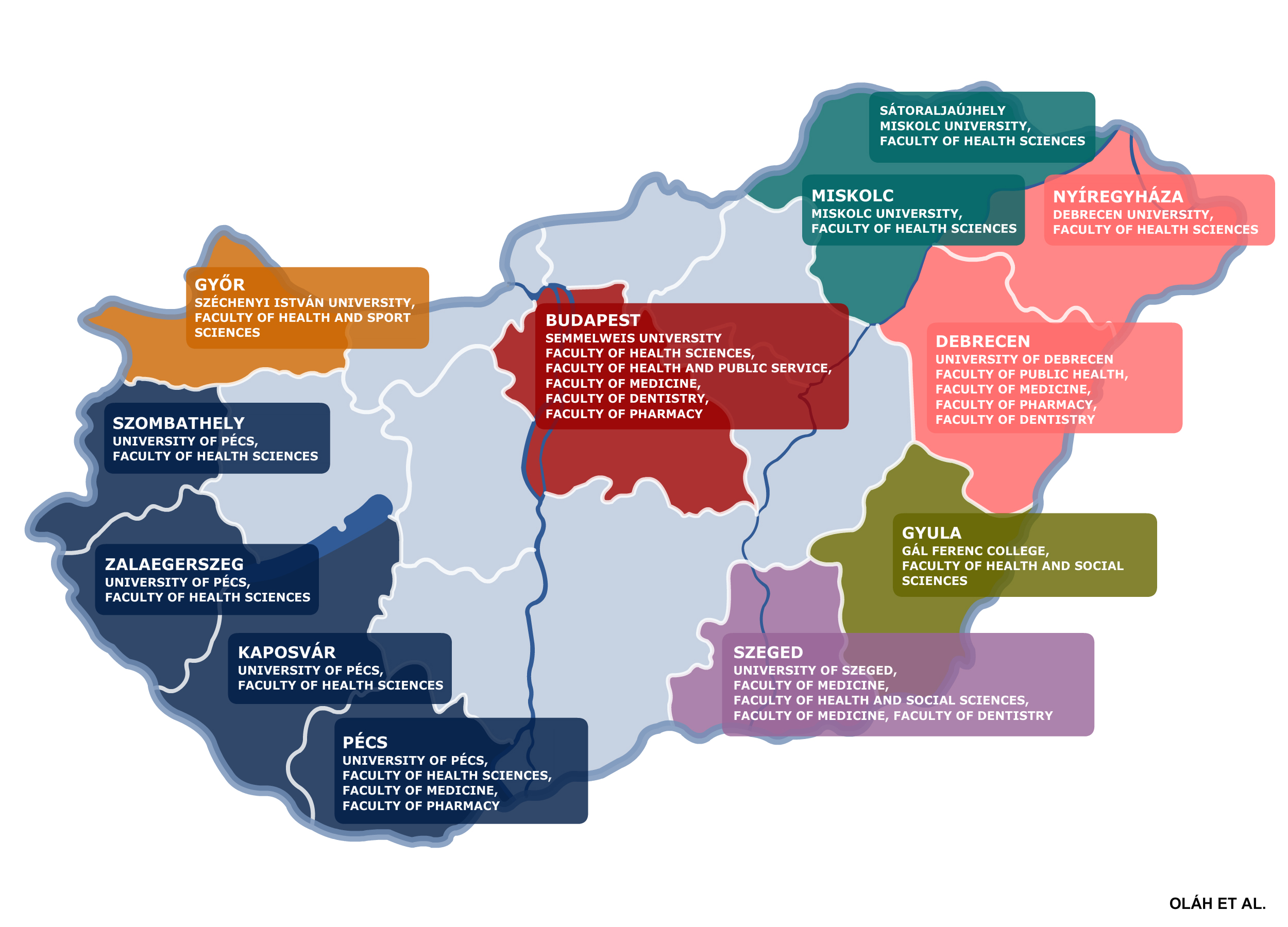
Figure 8: Locations of medical - and health sciences related higher education institutions in Hungary
Currently, there are 12 cities in Hungary (listed in alphabetical order: Budapest, Debrecen, Győr, Gyula, Kaposvár, Miskolc, Nyíregyháza, Pécs, Sátoraljaújhely, Szeged, Szombathely, Zalaegerszeg) conducting health care related educational programs (Figure 8).
For the most part, these higher educational institutions possess exploitable real estate- and human resources capacity, as they were able to educate/train a significantly higher number of students. It is recommended to organize health sciences educational programs in the social sciences educational establishments, or at other, already functioning locations in the form of a vocational educational institution (by locality of internship) of the higher educational institution. This structure holds several advantages:
After the regime change, the – not sufficiently grounded and not comprehensive regarding all levels of education – changes in education did not bring the expected results. In recent years, the number of people choosing career in health care continued to decline (Between 2014 and 2017 30% less health qualifcations were obtained and unfortunately, there are qualifications among health care qualifications that got promoted, which do not solve problems of shortage areas (especially nurses). While there are currently 5000 individuals are finishing health care vocational training on a basic level (not including the vocational high school students) and there are approximate of 1900 individuals qualify annually as a practicing nurse and 1300 individuals as nurse, 250 individuals as Bachelor nurse, in case of the realization of the concepts of the current care strategy, a minimum
Among others, aiding the solution of the nursing human resources crisis, the job-creation of lagging regions, the gradual improvement of individuals enrolled in lower educational levels, and the significant improvement of patient care quality. Main elements of the recommended education-development (Figure 9).
Summary: In addition leaving unchanged the number of hours during school years (according to EU Directive 2005/36, only those hours can be calculated which were completed after the 10th grade) and adding the 1191 hours of 11th and 12th grades (604 theoretical hours, 152 hours from the group of optional subjects and 587 practical hours, in which 280 hours is one tier practical internship) and the 2-year long associate degree’s 2240 hours of education built on the high school degree (theoretical: 1070 hours; practical: 1170 hours), the EU’s 4600 hour-long directive can be completed within 3431 hours (theory: 1674 hours, practice: 1757 hours), because the EU directive allows the counting of individual preparation with the use of ECTS, thus the missing 1169 hours can be specified as individual preparation (as it happens in the case of international practice). The directive also states that nursing education can only be organized as a full time, school system education, with these conditions the concept meets. In addition, as an associate degree the professional structure can be included in higher education up to 90 ECTS.
Conditions for admission: minimum age: 16 years, primary education, basic competences and skills required for finishing primary school (writing, reading, counting, self-performed grammar and arithmetic operations related to everyday life). The education can be carried out as part of the general nursing and health care assistant education in vocational schools or as part of bachelor nursing education, or independently. At the same time, it is necessary to examine whether the provisions of the Act XXXIII. of 1992 on the status of public servants should be amended according to the implementation in health care institutions (356/2008. (XII. 31.) Government Decree) in order to enable employment at the age of 16. According to the Act on the Status of Public Servants Article 20 (2) of the Act XXXIII of 1992 contractual relationship with a public servant can be set up with an “…at least 18 year-old…etc” person. However, the law on the implementation in medical institutions 356/2008. (XII. 31.) Government Decree, Section 2 (1) in contrast with the Act on Public Servants Article 20 (2) (b) to fill a position that requires a health care professional qualification a person who has not reached the age of eighteen may also be employed as a public servant, if the public servant at the time of establishing a public servant relationship is educated to get the required professional qualifications and skills. The education of qualified assistant nurse education is recommended to be conducted aside from faculties of health sciences and public educational institutions, by health institutions and national institutions involved with skill development. Below we propose lectures and the amount of educational hours of qualified assistant nurse education, taking into account the international practice (Table 1).
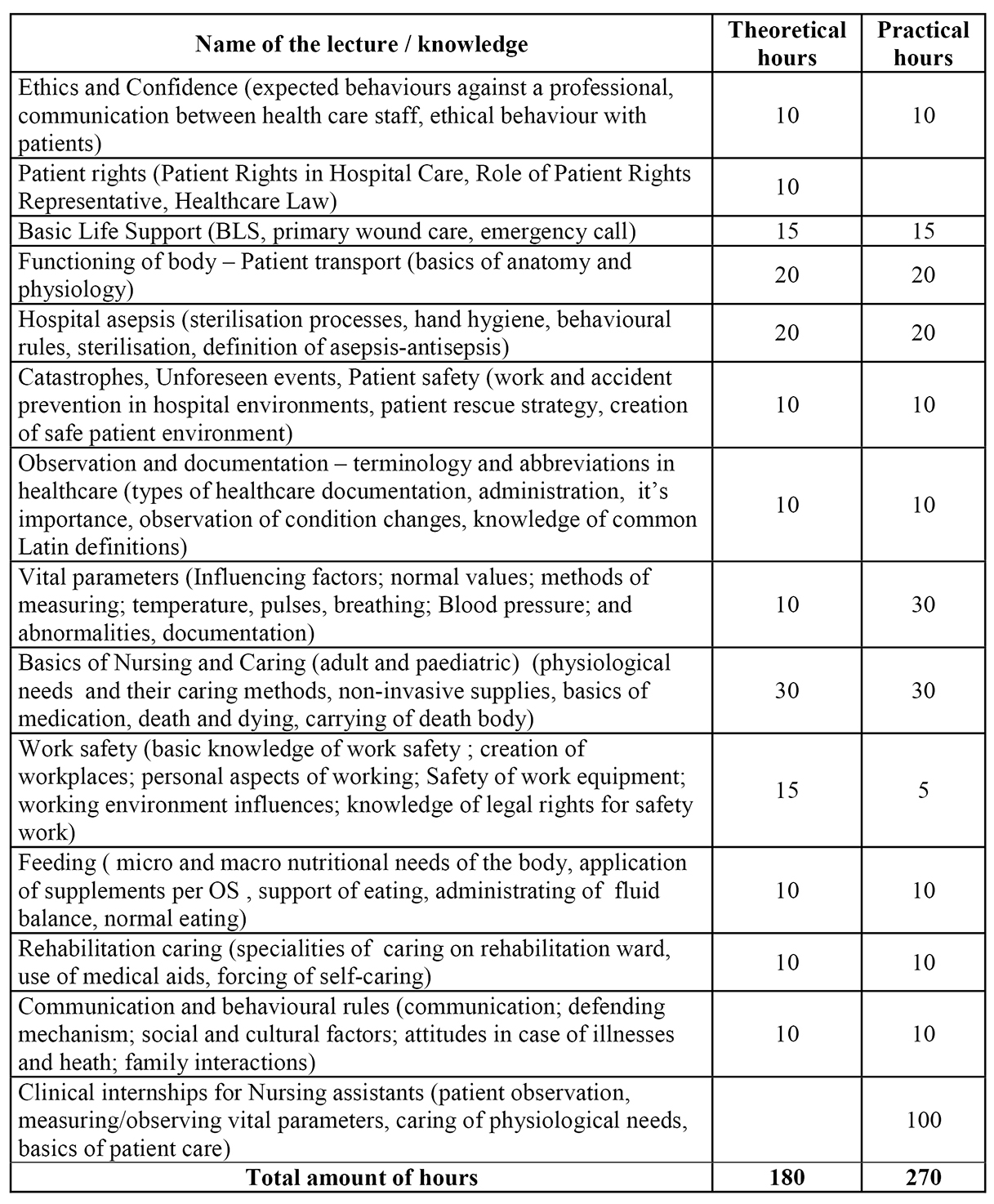
Table 1: Proposal lectures and the amount of educational hours of qualified assistant nurse education, taking into account the international practice79, 80, 81, 82, 83, 84, 85