There is a shortage of nurses in Hungary, the nursing system portrays an aging image and the resupply as well as the excess number of individuals necessary for the increasing demands cannot be provided. The average number of nurses per 100000 population in Hungary is low compared to the European Union average (75,7% in 2014). It is also lower in the WHO European Region (including Russia, Uzbekistan etc.) average (88,7% in 2014) as well. According to the analysis of the Hungarian Health Care Professional Chamber (MESZK), the number of nurses working in Hungarian healthcare was 26 thousand less than the required number in 2014. In our country, the number of newly recruited nurses in 2016 was decreased by 757 individuals compared to 2015 (from 1681 individuals in 2015 to 924 individuals), i.e. by 45% (which is the lowest degree for a long period of time in the past). The situation is further worsened by the fact that although the number of qualified nurses – along with the vocational education – has been continuously rising between 2009 and 2014 – followed by a repeated decrease by 10% until 2016 –, the number of qualified and newly degree nurses fall under the number of the qualified workers on a rising extent annually, in the past three years only 50-60% of the qualified workers were recorded in the operational registry.
It is a typical problem that there is a lack of available data to nurses. According to their numbers or their population pyramid data and analyzations, development recommendations based on them are unknown. Regarding the population pyramid, it might be instructive that based on the age-distribution of health care professionals (majority of them are nurses) it can be determined that 49% of the complete staff works within the 35-49 age bracket, while 32% works in the 50-69 age bracket. The 19% ratio of health care professionals under the age of 34 is a notification for the health care professional- and within that the nurse profession-representatives’ aging and reduction.
The validity of the data is questionable and only utilizable for trend-analysis, as an inquiry from the basic- and operational registry database and their numbers unfortunately provides data which differs from the actual professional/nurse number by thousands of individuals. Multiple displays of certain professionals or even a lack of names is a common error, as well as databases displaying the text “unknown”. Sometimes this text is displayed at the address, the issuer of the diploma, the postal code and the settlement simultaneously. These data clusters in such a form render the screening of duplication impossible. Also, regarding both the national (e.g. basic and operational registry, OSAP), and the international (e.g. HFA-DB, OECD) data services, the definition of the term “nurse” show significant differences, distorting statistical data to different degrees. In certain data bases midwives or even assistants are listed in the nurses’ group. The lack of consistent terminology makes the validity of the data doubtful and this way, they are only suitable for trend-analysis.
Figure 1 from the Organisation for Economic Co-operation and Development (OECD) source shows that there is a small difference between the numbers of physicians per 1,000 inhabitants (the average is 2-4 physicians per 1,000 inhabitants in the countries). Hungary is close to the OECD average. However, we are far behind the OECD average in term of the number of nurses. On the issue of human resources in economically developed countries where the health care system is well developed, they clearly contributed to raise the quality of services by increasing the number of nurses. This can be the breaking point!
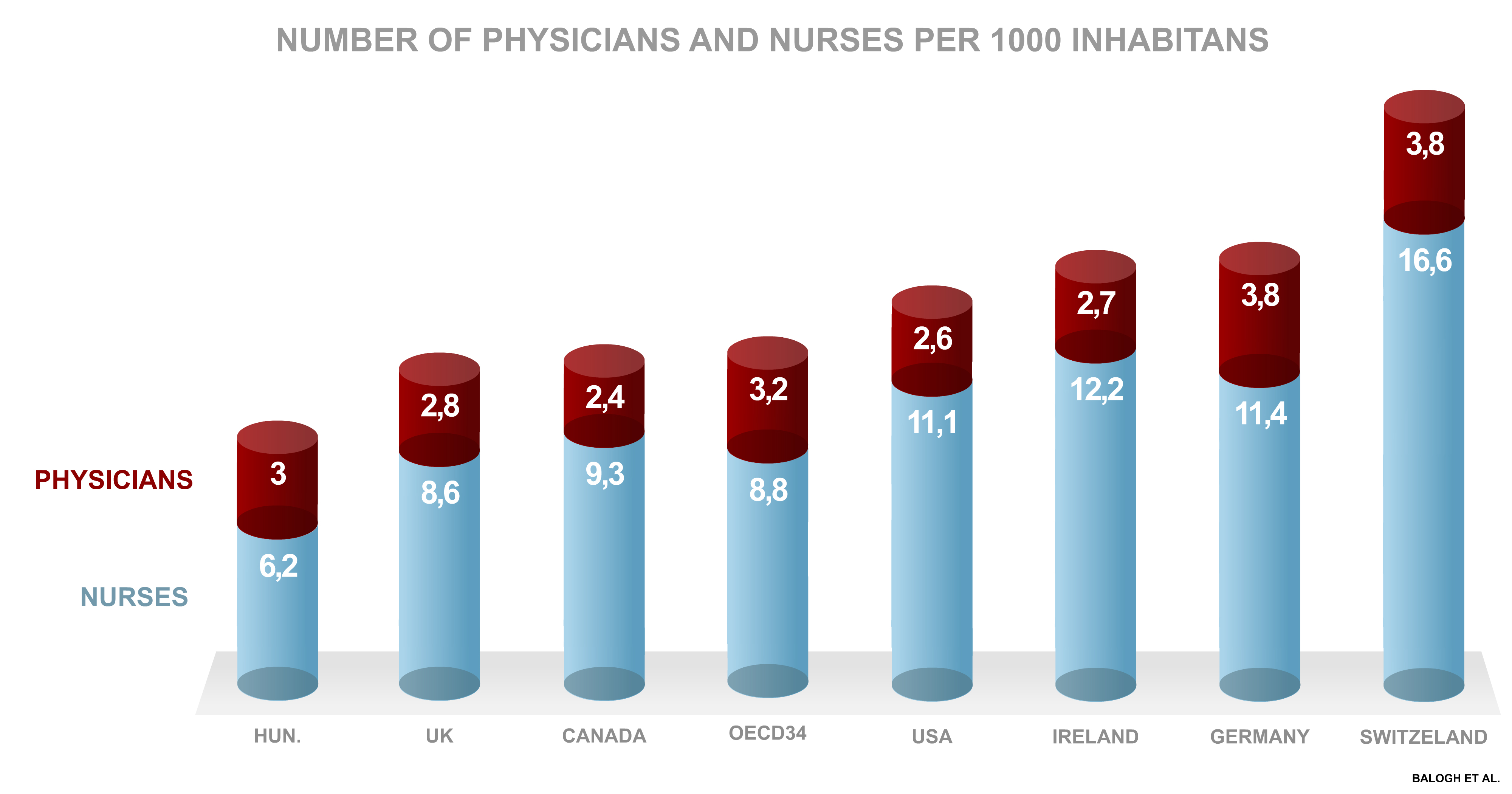
Figure 1: Comparison of physician: nurse ratio per 1000 inhabitants in the different countries
The OECD report from January 2019 on the economic performance of Hungary also clarifies that the aging society will not be the only be a challenge for the pension system in Hungary, but also to the health care system. The report argues for the inevitable change in the structure of healthcare system due to the aging, in which acute care is imagined to be practiced in less and professionally more concentrated hospitals. It emphasizes that the unbalanced availability of health care should be shifted to primary and outpatient care, which would strengthen the definitive preventive care function of primary care. The material indicates negative trends in labor supply regardless of health, which, of course, is also a symptom of crisis in healthcare, not only among physicians, but also among nurses. Last but not least, the report continues to show low wages, wheather we investigate this issue in comparison with German-Austrian or Czech-Slovak-Polish data.
All these macroeconomic and social processes call for the need for a national strategy at health policy level to provide short- and medium-term responses to the problems identified through the renewal of nursing services and education. Here the fact should take into account that Master nurses with advanced practice should be given a prominent role in acute care, which is shifted to primary care, whose competence allows basic access to health care in disadvantaged or unpaid GP practices. Their roles are expected to increase as a result of the lack of physicians and health visitors in settlements with beneficiary status (formerly disadvantaged). It would be necessary to settle nursing staff (shortage) in order to have an adequate number of nurses with the adequate educational level to effectively deal with the problems of an aging society, either with the extension of professional home care and telemedicine systems, either with the introduction of an assisted lifestyle community service, which is already tried and tested in the USA, or with the introduction of “transit”, temporary care wards that take the burden off the shoulder of acute care. The report clearly demonstrates that the number of avoidable hospital admissions is twice as high in Hungary as the OECD average because of e.g. asthma and COPD, which can be reduced to the OECD average with the adequate nursing care. It should not be forgotten that, as the Hungarian society as a whole is aging, future nurses will not be an exemption from it either, therefore special emphasis should be placed on improving working conditions (to make nursing career attractive at all, or at least to keep the current staff) and the widest possible use of robotics and artificial intelligence (patient lifting robots, remote monitoring systems, etc.). Last but not least, referring to the report’s findings on wages, if the wages of nurses are significantly below the Austrian-German labor market’s average, due to the possibility of emigration, the gap in nursing deficiency will increase despite all our efforts.
As a way of remedying deficiencies, our work group made an attempt to rectify the problems in the operational registry stated above – with our humble tools – and to acquire data reflecting the actual facts the most. Our research concluded that, that there are 39572 individuals with qualifications on different levels of nursing in the operational registry, and 29899 individuals out of these possesses nurse (Nurse/Infant- and pediatric nurse/ vocational level/, Nurse /Bachelor level/, Nurse /Master level/) qualification. We can only manage this data with certain reservations as well and we hereby would like to draw particular attention to the problem related to the data. Aside from that, we believe that by remedying the problems of the operational registry, the data demonstrated below will be clarified as well.
Based on the minimum requirements such as the number of nurses and the required qualifications in the 60/2003. (X.20.) ESzCsM Decree (Minimum decree) we found it important to transform the staff needs, which are needed to be developed in short, medium and long term proposals, based on methodology and international good practice.
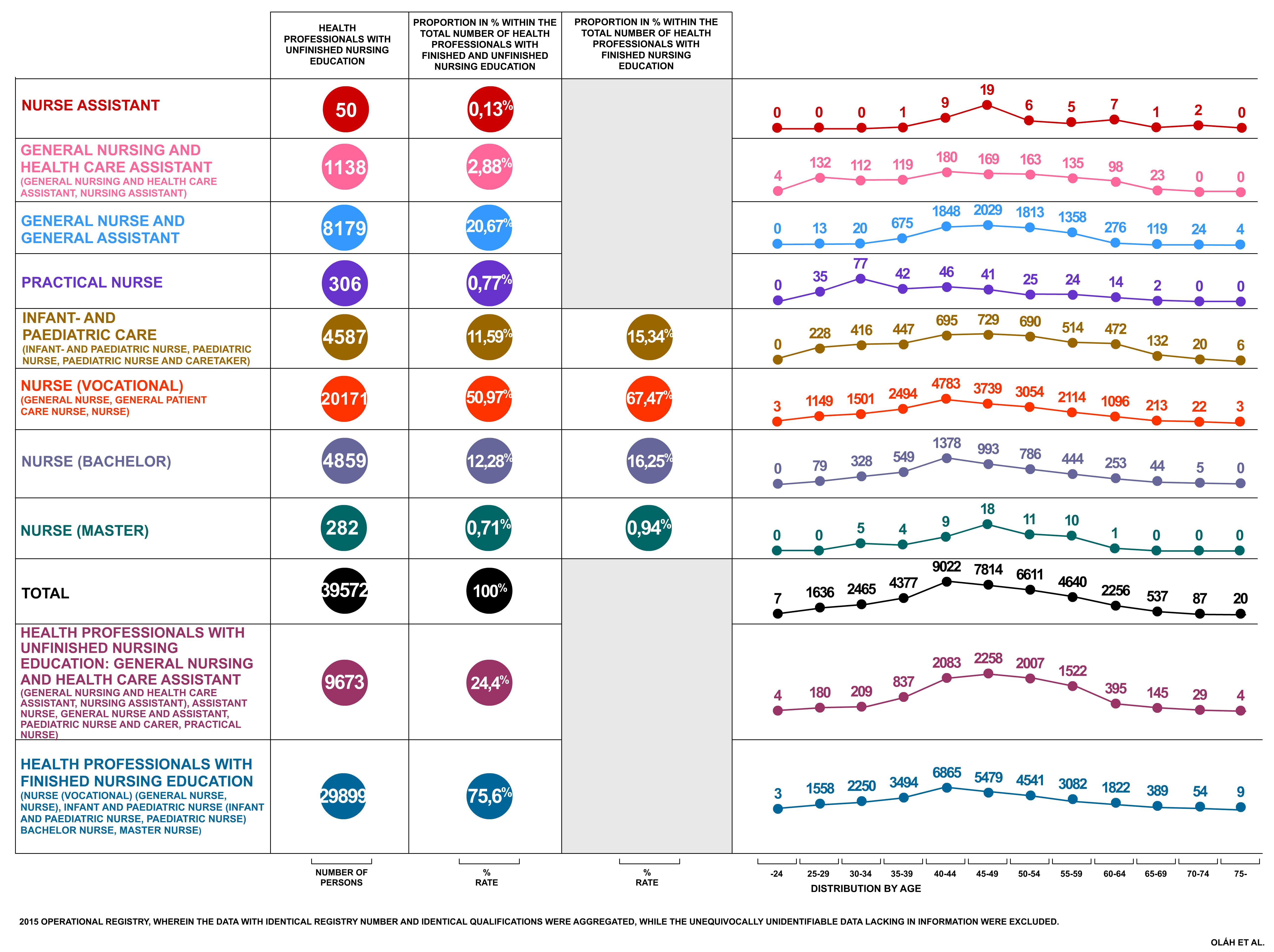
Figure 2: Number and age distribution of nurses with different qualifications
In parallel, we processed data contained in the register of operations per institution, then also at county level relating to professionals with nursing qualification and professionals without finished nursing qualification (Figure 3, 4, 5, 6).
If we want to decide the number of nurses working in inpatient and chronic care, from this number we need to deduct the number of nurses who are in the operational register, but work in the primary care, outpatient care/occupational care/social care.
In the register of operations 2015 we can find 9673 professionals without finished nursing education and 29899 nurses with finished nursing education.
Additionally, county breakdown data may be distorted by the fact that nurses are not currently employed int he same county where their zip code is listed, also it is important to know that due to the expiration of the 5-year period of operational register, many colleagues who have left the career path, retired, etc. and does not extend its operational records will ereased from the system. The authors of this paper only wanted to report this data as a baseline in order to draw attention to the problem by asking for a broad cooperation on the basis of the appropriate methodology and data provision on nursing deficit by institutions and countys.
As far as we know, the Association of Hungarian Nursing Directors and the Chamber of Hungarian Health Care Professionals have research results on the subject, of which, with the results of this study, it can help to form an accurate picture of the situation. This can be the only basis for developing short-, medium-, and long-term education and employment system based on a realistic picture. Only the above mentioned can form the basis of a realistic picture on forming short-, medium-, long-term education (scholarship) and employment system. There is a need for an urgent, well-thought-out, immediate and short-term (and solution-giving) concept, and at the same time, the development of a concept suitable for achieving medium and long-term goals should not be eliminated. Creating the exact picture of position will not only help to solve the anomalies of the operational registry. At the same time, the relevant data are still available and the analysis and publication of the data of the Registry of Human Resources’ (Humánerőforrás Nyilvántartó Rendszer, HENYIR) database is also highly justified. In this system, health care institutions must provide data about health care workers, “…who is qualified to carry out the health care activities, or someone who is not qualified, but contributes in tasks performed by qualified health care professionals”. They must record the names of the employees (name in EEKH), FEOR number of the scope of activities, scope of work, start date of employment (if its possible also the planned end date, for fixed-term contracts) full- or part time employment, form of work, the duration of volunteer over-time work and the reason for permanent absence.1 In any case, the data must be recorded by the employer, even if the employee is for example in an individual entrepreneur status, because in this case this is the legal relationship. At the same time, in the case of a “redundant” worker, the supply of data should be made by the employer agency. If workers work in more than one unit, they must be listed for each units. Only those workers who actually provide health care should be included (bedside workers), for example the informational desk workers and those who participate in education must be excluded. The maximum amount of weekly work hours is 60 hours, the weekly hours of on-call time do not count. If a worker works in more than one unit than the weekly working time must be given to each units. If a nursing assistant has an EEKH registration number then the 3311 nurse, professional nurse FEOR classification should be given, if the nursing assistant does not have it, they should not be added to them system.
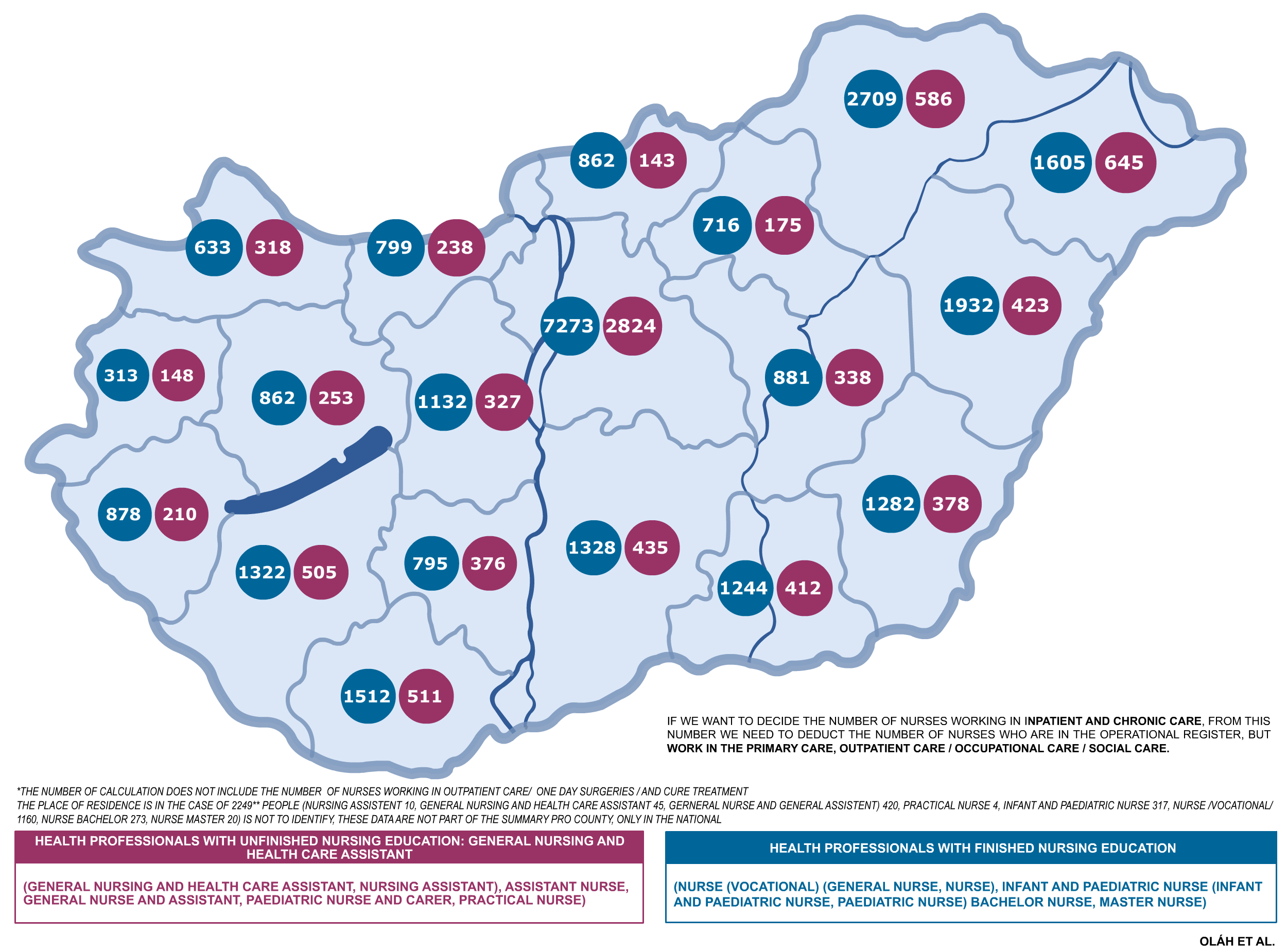
Figure 3: Number of professionals with and without finished nursing education, according to the register of operations (corrected by the number of nurses whose address can not be identified in the operational register because of the absence of postal code), broken down by county

Figure 4: Allocation of professionals with finished nursing education according to the register of operations (corrected by the number of nurses whose address can not be identified in the operational register because of the absence of postal code), broken down by age groups and counties
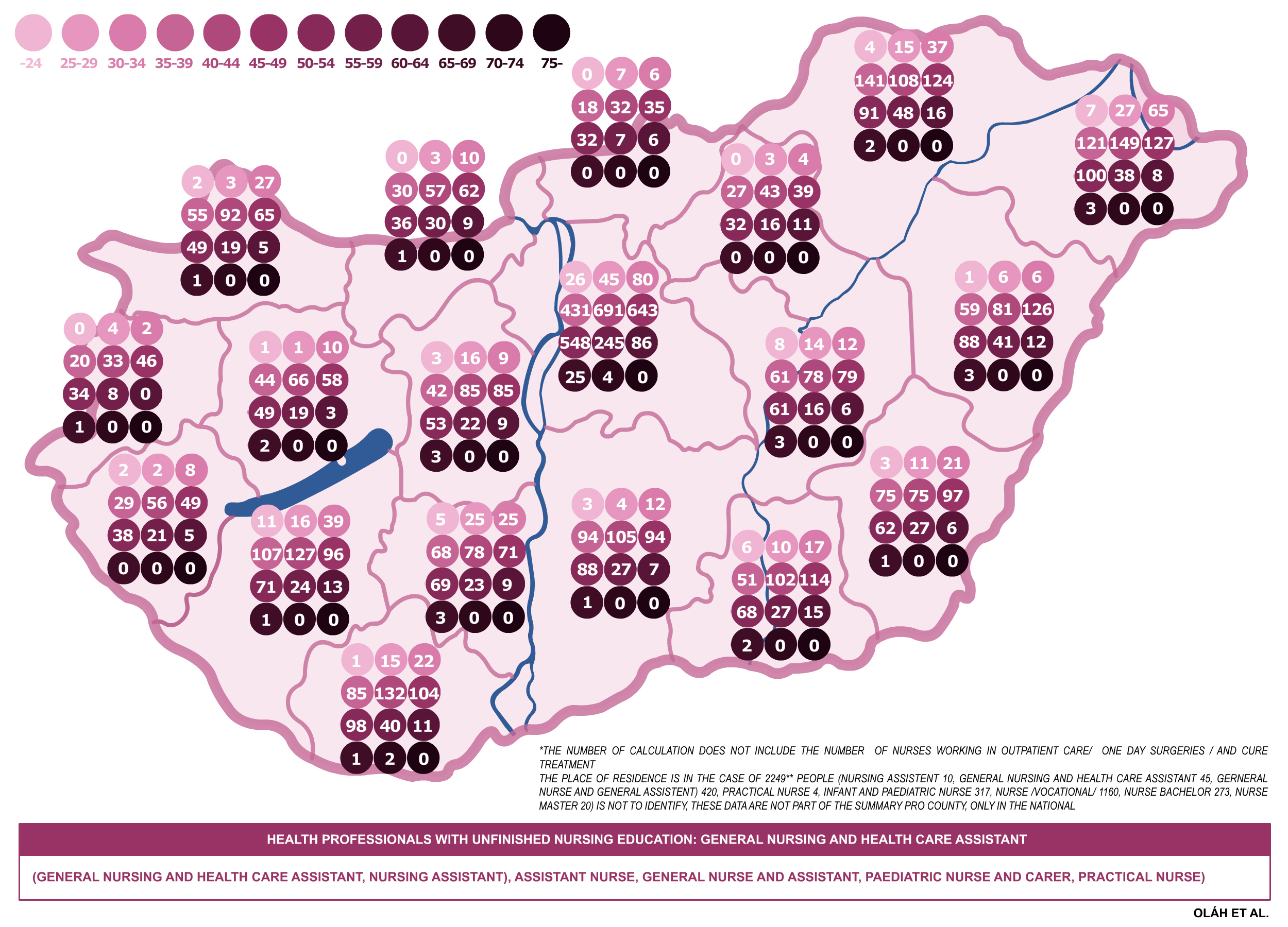
Figure 5: Allocation of professionals without finished nursing education according to the register of operations (corrected by the number of nurses whose address can not be identified in the operational register because of the absence of postal code), broken down by age groups and counties
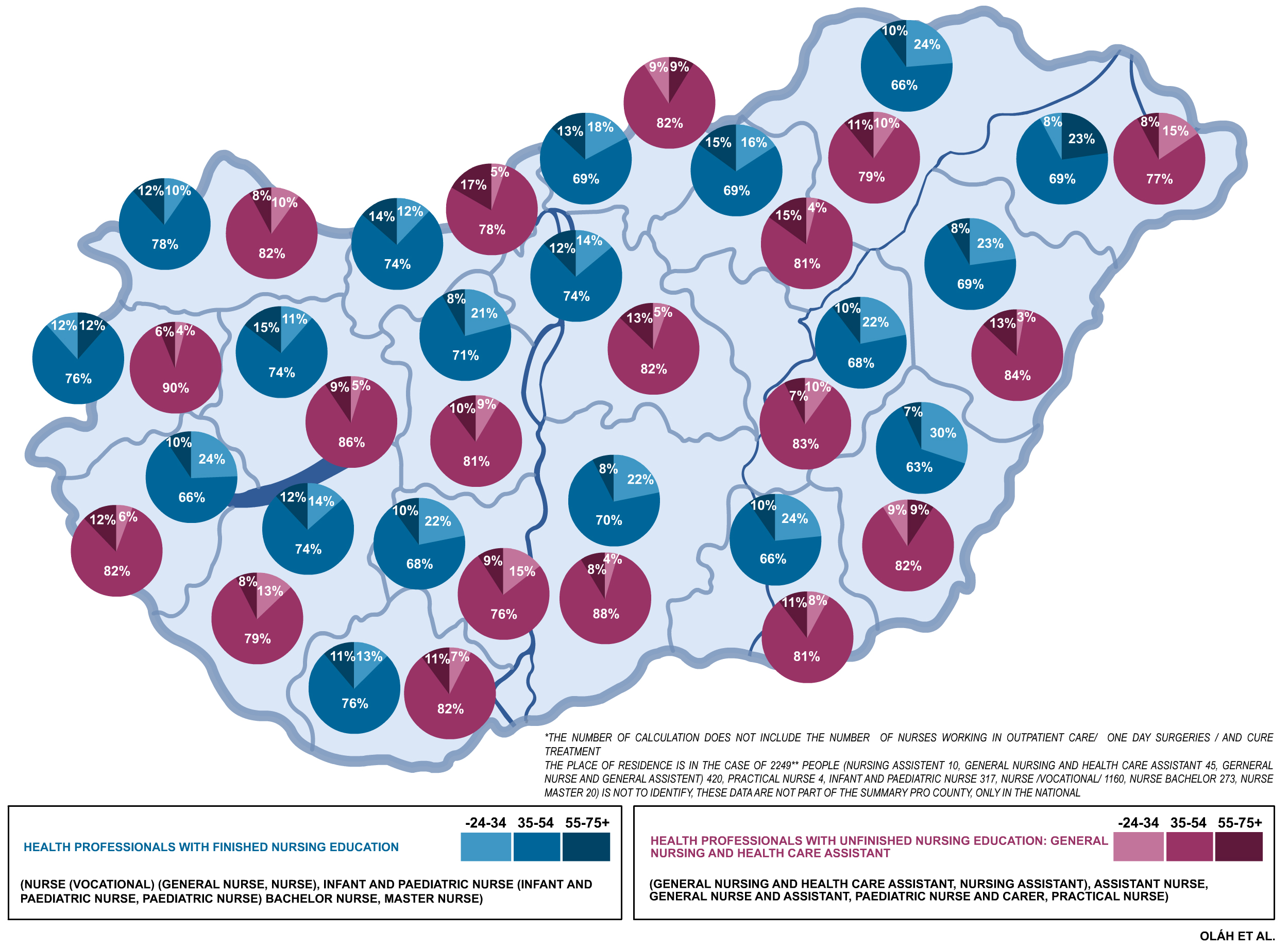
Figure 6: Allocation of professionals with and without finished nursing education, according to the register of operations (corrected by the number of nurses whose address can not be identified in the operational register because of the absence of postal code), broken down by age groups (%) and counties